63Y/M with right sided abdomen pain
63Y/M with right sided abdomen pain
6/2/22
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box.
A 62 year old male patient , Carpenter by occupation came with complaints of Right sided abdomen pain ( 4 days back ) with diffuse chest pain
History of presenting illness
The patient was apparently alright r days back then he developed on and off right sides abdomen pain which was not associated with vomiting / loose stools
Relieved on taking medication
A day before yersterday morning around 3 am patient had a pain in right side of abdomen not relieved on medication radiating to back and right shoulder and right upper limb it was associated with one episode of vomiting not associated with sweating or heaviness in chest
PAST HISTORY
Not a known case of Hypertension , diabetes , asthma , TB , epilepsy.
The patient had a tooth extraction 1 month back because of tooth pain he took some bland and smooth diet . he decreased food in take from 4 days back because the patient experiencing more pain in abdomen after taking food
PERSONAL HISTORY
Appetite - normal
Sleep - disturbed ( because of pain)
Bowel and bladder - regular
Addictions - takes alcohol daily
Chronic alcoholic - takes 90 - 180 ml per day, some times skips ( rarely) since >20 years
Chronic smoker also - takes 1 pack( 10 - 12) of cigarettes/ bidi per day since > 20 years
FAMILY HISTORY
No significant family history
GENERAL PHYSICAL EXAMINATION
Patient was conscious , coherent , co-operative , moderately built and nourished , well oriented to time place and person
Pallor - present
Icterus - absent
Cyanosis - absent
Clubbing - absent
Lymphadennopathy absent
Edema - absent
SYSTEMIC EXAMINATION
•Abdomen examination :
On Inspection - abdomen was slightly distended , no engorged veins , scars sinuses
- umbilicus : central
On Palpation - the right hypochondrium was very tender and resistance was felt
And the patient was not allowing to palpate the abdomen because of the pain .
On Auscultation - bowel sounds was heard
CVS : S1 , S2 heard no murmurs
Respiratory system - trachea was central , bilateral symmetrical expansion of chest was seen , normal bronchial vesicular sounds are heard , no stridor or crepitus
CNS examination
No focal neurological deficits
INVESTIGATIONS
USG
On USG 2 calculi noted on gall bladder of size 12 mm each
Gall bladder was thickened






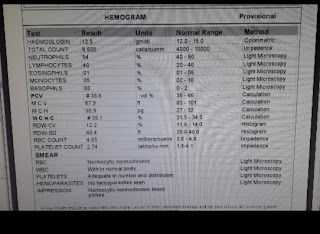
CBP - HB :- 13.5
TLC :- 13,600 cells / DL
Platelets :- 1.83 lacks
CUE-
Pus cells :- 2 - 3 cells
LFT -
TB :- 1.54
DB :- 0.88
SGOT:- 37
SGPT:- 10
ALP:- 144
Albumin:- 2.9
RFT-
S. Creatinine :- 1.1
Na+ :- 133
K+ :- 4.1
Cl - :- 102
Bloodurea - 23
RBS - 96 mg / DL
Troponin :- negative
Serum Mg+2 :- 2.1
DIAGNOSIS
ACUTE CHOLECYSTITIS with CHOLELITHIASIS .
TREATMENT
After admission the patient was diagnosed with hypertension
Patient was advice's not to take food till further orders
INJ NS
RL } 75ml/hr
DNS
INJ TAXIM 1mg /IV / BD
INJ tramadol 1 ampule / 100ml
INJ zofer 4mg /IV/OD
INJ PAN 40mg/ IV/OD
INJ AMIKACIN 500mg IV BD
INJ METROGYL 100ml /IV / TID
Adviced to give
INJ PARACETAMOL 1 gm IV sos( if temp > 101° F)


Comments
Post a Comment